

Psychopathy and Sociopathy
Are they the same thing, and are they both ASPD?

Where do you draw the line between psychopathy and sociopathy?
I hope you were looking for a super long answer, because that’s what you got.
About the same as I think about both of them being equated with ASPD. It’s a quagmire that could have been prevented, but wasn’t, and now we have a mess.
I get comments all the time about how psychopathy and sociopathy are “no longer terms”. That they aren’t used anymore, and using them demonstrates my lack of knowledge. I find this position to be rather strange, and at a minimum, ignorant. They are relying on the DSM to tell them what is considered “real”, when in reality, that’s a nonsense position. The terms are both very much alive and well, and psychopathy at least is heavily researched separately from ASPD. Why? Because it isn’t the same thing.
This wouldn’t be too much an issue if it weren’t for the people making these comments are often those that claim to be therapists, psychologists, people that should know better. They have credentials and the DSM in hand which apparently means that they believe they don’t have to put in any further effort. It’s… vexing. I ran across an answer from 2015 that speaks about this clearly;
“The DSM (the Diagnostic and Statistical Manual of Mental Disorders) is just terrible, and any mental health professional who thinks the DSM is "good science" should be considered with skepticism.
The primary purpose of the DSM is to provide numerical codes that doctors can write on receipts so that medical insurance can reimburse them. However, the DSM also needs to include rules for who qualifies for each numerical code. This is a fine purpose and the DSM serves this purpose as well as can be expected.
The DSM is not what researchers use to diagnose patients for inclusion in (or exclusion from) a clinical trial. Researchers have their own sets of criteria, and they evolve faster than the DSM, and with more scientific input.
The DSM-5 dropped the diagnosis of Asperger's syndrome, but the number of research papers about Asperger's syndrome has only declined partially. You can't write it on a medical bill, but you can still write a scientific paper about it.
It is best to ignore the DSM, unless you are writing a bill and you want to get the bill reimbursed.
In fact, many doctors who write DSM-5 codes on their bills do not use the criteria from the DSM-5 when making their diagnosis. They use other criteria, hopefully better criteria, but maybe worse.”
Onto sociopathy being conflated with psychopathy. If we can’t pull either one of them out of the mess of the DSM where they have basically removed sociopathy, and up until a very recent edit psychopathy (“psychopathic features”) as well, and we have people still believing that the DSM is a bible of all things going on in the brain, it stands to reason that the conflation is going to continue unabated for some time.
The answer above speaks about something that most people miss. Something not being listed in the DSM does not remove its existence from reality. It’s an inconvenient truth to be sure, but that’s how it is. I think that there is an argument for sociopathy to be in the DSM. It is theorized to be genetically rooted, but largely is environmentally caused. If it is an adjustment to the world based on environmental factors including severe abuse, neglect, or long-term trauma. I think that is something that should be dealt with in the realm of psychology.
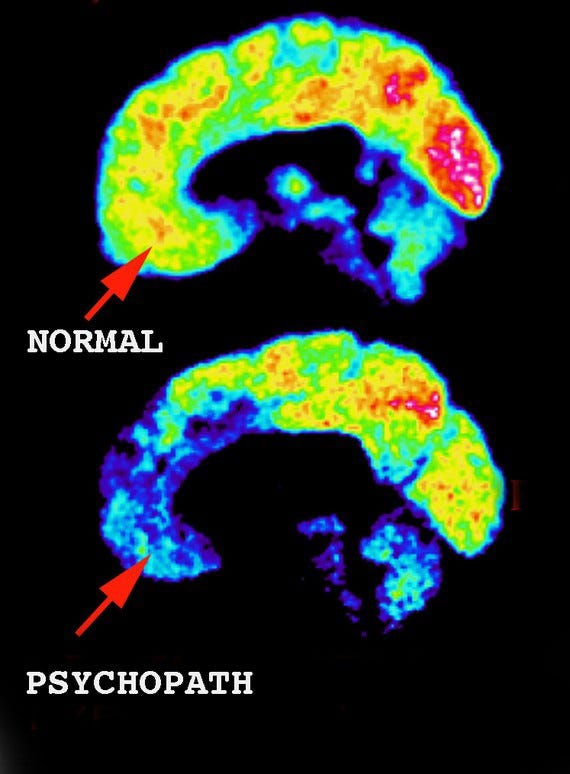
However, the same argument cannot be made for psychopathy. Psychopathy is genetic, it is not environmental. What changes in a psychopathic person based on environmental triggers is behavior, not the psychopathy itself. Regardless of how a psychopath is raised, they are born psychopathic, and psychopathy will remain. Environment and abuse can create a very badly behaving psychopath, but won’t make them more or less psychopathic. Scan the brain of a noncriminal psychopath, and you will see what I mean;
Look at the synaptic connections, and you will also see what I mean;

Connectomes—mappings of neural connections in the brain—showing differences in connectivity between the neurotypical brain, the high-functioning autistic brain, and the psychopathic brain. (Image credit: Walt Schneider, University of Pittsburgh, and Human Connectome Project
Sociopaths on the other hand don’t seem to have structural differences in the brain. Perhaps there are changes, but so far, that hasn’t been demonstrated. Due to this, sociopathy gets the shaft in terms of research. If you can’t point to something and say, “See, there it is”, no one wants to give you research money to look into it further. Psychopathy has differences that can be mapped, sociopathy so far, doesn’t.
When they get conflated it adds to the proverbial shafting that sociopathy is already getting. Whether people like it or not, psychopaths and sociopaths do not experience the world even slightly similarly. People get very up in arms about me stating this, but it’s factual.
Take a look at this;
“Sociopaths tend to be nervous and easily agitated. They are volatile and prone to emotional outbursts, including fits of rage. They are more likely than are psychopaths to be uneducated and live on the fringes of society. They are sometimes unable to hold down a steady job or to stay in one place for very long. It is often difficult, but not entirely impossible, for sociopaths to form attachments with others.
Many sociopaths are able to form an attachment to a particular individual or group, although they have no regard for society or its rules in general. Therefore, the meaningful attachments of any sociopath will be few in number and limited in scope. As a rule, they will struggle with relationships.
In the eyes of others, sociopaths will generally appear to be disturbed or erratic. Any crimes they commit, including murder, will tend to be haphazard and spontaneous rather than planned. Because of their seemingly erratic behavior, sociopaths are easier for both professionals and nonprofessionals to identify than are psychopaths.”
As opposed to;
“Unlike sociopaths, psychopaths are unable to form emotional attachments. Psychopaths tend to be aggressive and predatory in nature. They view others as objects for their amusement. Although they lack empathy, psychopaths often have disarming or even charming personalities. They are manipulative and can easily gain people’s trust. They learn to mimic emotions, despite their inability to actually feel them and will appear normal to unsuspecting people. Psychopaths are often well-educated and hold steady jobs.
Some psychopaths are so good at manipulation and mimicry that they have families and other long-term relationships without those around them ever suspecting their true nature. When committing crimes, psychopaths carefully plan every detail in advance and often have contingency plans in place. They will seem unflappable in a crisis.
Unlike their sociopathic counterparts, psychopathic criminals are cool, calm, and meticulous. From a law-enforcement perspective, the “cold-blooded” nature of psychopaths makes them very effective criminals. As such, they are generally more difficult to identify than are sociopaths. Unfortunately, it can be hard to know when a psychopathic predator has targeted you for exploitation.
From a diagnostic standpoint, the etiology or cause of psychopathy is different from that of sociopathy. I contend that psychopathy is the result of “nature” (genetics), while sociopathy is the result of “nurture” (environment). Psychopathy is related to a physiological defect that results in the underdevelopment of the part of the brain responsible for impulse control and emotions (1).
Sociopathy, on the other hand, is more likely the product of childhood trauma and physical or emotional abuse. Because sociopathy appears to be learned rather than innate, sociopaths are capable of empathy in certain circumstances, and with certain individuals, but not others.”
Now, do I agree with everything that he said? No, of course not. The description leans hard into the idea of criminality associated with either one. He also makes the claim that psychopaths are aggressive and predatory in nature. That is rather hyperbolic and misleading, or at the very least treats the criminal class as the standard. It’s unfortunate, but all the research studies are done in prisons, so we have to take what we can get in terms of information. What this does show though is fundamental differences in how sociopaths and psychopaths are, yet people say that they cannot be differentiated from one another.
To say that they are the same, or to say that either term has no current value because the DSM says so is misinformation. I do not like misinformation, it annoys me. I also do not prefer people that apparently practice in the mental health field telling me that they are outdated terms. It makes me think that they do not do any reading to further their education. I have heard from people that have degrees in psychology who state that their entire education in abnormal psychology was a day.
One day. That is the in-depth education that they get on all abnormal psychology, and unless they have furthered their education on their own or have gone on to specialize in abnormal psychology. That is the amount of information that they are objecting to my answers with. One. Day. This sort of thing, however;
“User
Over inclusivity does not create clarity in fact the intent is to distort which is common among those in denial. Youve posted a lot of drivel. Its a genetic disorder with no cure and often the best treatment is a long prison term for many of them. They are very easy to identify after having worked with many of them over the past 25 years. At times they can even be amusing.
Athena Walker
Original Author · Apr 23
I find it fascinating that you consider science to be drivel.
You stated;“The very last person we should ask about this disorder is one who has it.” And that would be fine if I didn’t have research, and science to back up what I say. You clearly don’t care, which is fine, that’s your prerogative. However, what I state is not rare, or incorrect. It is well backed and researched. You may disagree with me, but disagreeing with the evidence I provided isn’t disagreeing with me, it is disagreeing with;
Is your child a psychopath? Study measures psychopathic traits in kids
Genetics of callous-unemotional behavior in children - PubMed
Genetics of callous-unemotional behavior in children - PubMed
Variant in oxytocin receptor gene is associated with amygdala volume - PubMed
The association between oxytocin receptor gene polymorphism (OXTR) and trait empathy - PubMed
Genetics of Callous-Unemotional Behavior in Children
Ten years ago today, it was revealed that the human genome had been
http://moritzlaw.osu.edu/osjcl/Articles/Volume3_2/Symposium/Fallon-PDF-03-29-06.pdf
Here's what a psychopath's brain looks like
Dissociable Effects of Serotonin and Dopamine on the Valuation of Harm in Moral Decision Making
Brain Region's Dopamine Levels Linked to Psychopathy Trait
Atypical nucleus accumbens morphology in psychopathy: another limbic piece in the puzzle
Reduced Prefrontal Connectivity in Psychopathy
Genes for susceptibility to violence lurk in the brain
to name just a few. Again, your choice, but it seems a strange one to make.
User
classic
Athena Walker
Original Author · Apr 23
Indeed, presenting evidence is classic. As is should be with anyone with academic rigor.
User
Or compulsive denial
Athena Walker
Original Author · Apr 24
Many of the faults you see in others dear reader, are your own nature you see reflected in them.
User
The old school projection defense. I m surprised it took you so long to put that one out there. I love this.
Athena Walker
Original Author · Apr 25
You’re surprised it took me so long to call you out on your behavior?
You don’t want to look at science, have not at all addressed the evidence that I presented to you, as it appears you are unable, and your response instead is personal insults. Fascinating.
User
Im just having too much fun not taking you seriously
Athena Walker
Original Author · Apr 25
It’s unfortunate that you don’t take science seriously, but that’s your choice.
User
Its you I dont take seriously.
Athena Walker
Original Author · Apr 25
No, it isn’t. You don’t know me. What I have told you is scientifically backed, and that has nothing to do with me as a person. That’s an unfortunate choice you have made, but not one that has any impact on me. Just you.”
is just a portion of a lengthy exchange with someone touting these credentials “MS in Counseling Psychology & Child Trauma”. There is no willingness to read the information, not consider something that contradicts their apparently rather entrenched view of things. If this is what can be expected from people in the field, it is no wonder that psychopathy and sociopathy are as entangled as they are.
How can you reverse the level of cognitive dissonance that the overreliance on the DSM creates? I have no idea. I write about it, people can disagree, that’s fine, but they should at least think about whether there is a reason to be so steadfast in this notion that psychopathy, sociopathy, and ASPD are exactly the same.
Think of it this way. Let’s say you have a psychology or therapy license, and you are just starting out. You have a slightly larger body of education in abnormal psychology than the average person, but still aren’t delving into the heavy research on psychopathy or sociopathy. Keep in mind that abnormal psychology is a lot of things, it isn’t going to be very focused on either one of the former particularly, as there is a lot of ground to cover.
Now you have a client that you think falls into the ASPD category. All right, cool. What are you going to do when this person that you think has ASPD, and even more specifically you think is psychopathic due to some of their history (believe it or not some professionals still think that normative humans don’t do awful things, they must have a disorder past simply being human) but your client doesn’t really fit the mold of a psychopath.
Perhaps they are obsessed with someone, have a very hot temper, have emotional triggers, can experience self-doubt, has a lot of markers of sociopathy, but sociopathy apparently doesn’t even exist. It’s just ASPD now. How are you going to approach that client? Are you going to just blindly nod and say, well the DSM says so, which means I don’t have to do any additional thinking? That would be a pretty crappy doctor, and yet this is exactly what a lot of people do
Add to this, the same amalgamation of things permeates the internet, so people come to me announcing with utter authority that they are exactly the same, and all listed under ASPD in the DSM. Therefore I am wrong, and have no idea what I am talking about. I present evidence, and I get the equivalent of;

That… is not a good look. Nor is this;
There is no such thing as a psychopath diagnosis. Its an old therm for personality disorders. There are a lot of them and they tend to mix in one person. So by telling that someone is a psychopath does not tell anything about that person. People with personality disorders do make suicide attempts. In lot of cases more often than people without them
That, that right there, it sums up everything wrong with this conflation, and by the way, I get comments like this all the time. None of that is accurate, but this is what people believe. Now, in fairness, this one is even worse than most, as it doesn’t even present the convoluted information accurately.
Let’s just concede for the sake of the argument that psychopathy should be considered a personality disorder. It isn’t, but let’s just pretend.
Psychopathy is not an old term for personality disorders. There are many personality disorders, and psychopathy at no time was a blanket term for all of them. Some people have components of different disorders, however, you aren’t going to have a psychopath that also has BPD, HPD, or NPD. However, you can have a person with HPD also have ASPD at the same time. The same is true for any of these because ASPD is describing behavior, not causation. Anyone can behave in a way that ASPD applies to them.
Do people with personality disorders commit suicide? Yes, of course they do. However, psychopaths really don’t. There isn’t a reason to, and part of being psychopathic is turning every situation into a bonus for me. Everything has a silver lining and psychopaths are absolute pros at finding how to make everything work to our advantage. Can I imagine a time that suicide would be the choice I would take? Sure. Give me a terminal illness with a long decline, and I will likely find a cutoff point where I decide I’m out.
Save for extreme circumstances, however, psychopaths don’t kill themselves. They have studied this, and psychopathy goes along with suicide resistance. This has been known since the seventies, but then along came the DSM and they mucked that all up. Take a look at this statement;
“H. Cleckley (1976) maintained that psychopaths are relatively immune to suicide, but substantial evidence exists for a relationship between antisocial deviance and suicidal acts. This study was the first to explicitly examine suicidal history among psychopathic individuals as defined by R. D. Hare's (1991) Psychopathy Checklist--Revised (PCL-R). Male prison inmates (N = 313) were assessed using the PCL-R and DSM-III-R and DSM-IV criteria (American Psychiatric Association, 1987, 1994) for antisocial personality disorder (APD), and they completed A. Tellegen's (1982) Multidimensional Personality Questionnaire (MPQ). Presence or absence of prior suicide attempts was coded from structured interview and prison file records. Suicide history was significantly related to PCL-R Factor 2 (which reflects chronic antisocial deviance) and to APD diagnosis but was unrelated to PCL-R Factor 1, which encompasses affective and interpersonal features of psychopathy. Higher order MPQ dimensions of Negative Emotionality and low Constraint were found to account for the relationship between history of suicidal attempts and antisocial deviance, indicating that temperament traits may represent a common vulnerability for both.”
Sigh. Do you know what the factor two traits are? They relate to ASPD, not psychopathy. In fact, even using Hare’s garbage rating scale that he stole the majority of from Cleckley, and somehow made it even less applicable to psychopathy than something cooked up in the 1940s, states “psychopaths (factor one traits) do not kill themselves, but people with ASPD (factor two traits) do.”
You know what else factor two traits relate to? Secondary psychopathy, which is a ridiculous label for sociopathy, which you can see here;
According to B. Karpman (1948), the primary psychopath can be described as:
“The root disorder in patients diagnosed with it whereas secondary psychopathy was defined as an aspect of another psychiatric disorder or social circumstances. Today the primary psychopathy is considered to have mostly Factor 1 traits from the PCL-R (arrogance, callousness, manipulative, lying) whereas secondary psychopaths have a majority of Factor 2 traits (impulsivity, boredom proneness, irresponsibility, lack of long term goals).”(Karpman, 1948, p. 525)”
“Other authors have noted that primary psychopathy is used “. . . to differentiate between psychopathy that is biological in origin and secondary psychopathy that results from a combination of genetic and environmental influences” (Mealey, 1995, p. 3).”
and;
“The terms psychopath and sociopath are often used interchangeably, but they aren't quite the same thing. So what's the difference, you ask?
To find out, we asked James Fallon, a neuroscientist at the University of California at Irvine School of Medicine who specializes in studying psychopaths (and also happens to be one himself).”
While neither term appears in the Diagnostic and Statistical Manual of Mental Disorders, the medical handbook used by psychiatrists, psychopaths can be divided into two categories, according to Fallon. The first category includes what are known as primary psychopaths. The second includes what are known as secondary psychopaths, or sociopaths.
Back to the suicide passage. You know what it demonstrates? It demonstrates the absurdity of the current state of things. It states psychopaths don’t kill themselves, but they do kill themselves because they are grouped under ASPD, but not the primary psychopaths. They actually don’t kill themselves, but the secondary psychopaths, which are also known as sociopaths, or just folks with ASPD, they do kill themselves at a somewhat higher rate than most. What they want you to believe is that they are exactly the same thing, but behave totally differently.
Just… what?
I think it’s a mess, and psychology has no one to blame but themselves. I don’t think that the DSM should be considered anything of real value unless you are attempting to extract repayment for services from an insurance company. I also think that the people doing the studies on psychopathy, sociopathy, and ASPD have created such a large clusterf*ck (as evidenced by the suicide quotation), that it’s unlikely to be sorted soon. Don’t forget to add into the mix the heavy reliance on the PCL-R as “reliable” and the “gold standard” for measuring psychopathy.
Tell me, how you are accurately diagnosing anything with a twenty question checklist that overly relies on criminality, and antisocial behavior, but somehow also diagnoses three separate and distinct things, psychopathy, sociopathy, and ASPD, that are also somehow all the same thing, but very very different at the same time? How is that tool remotely reliable? It has to be broad and overreaching to even attempt to make that happen, but it’s the “gold standard”. How does that work exactly? Not well, that much I can assure you.
Maybe people will reconsider in the future, and better information will be out there to make it easier to understand. As long as Hare is around, and the DSM is held in such high regard, I very much doubt it. For now, we are stuck in the trainwreck of it.
Life as a Nonviolent Psychopath
The Differences Between Psychopaths and Sociopaths
Psychopathy, antisocial personality, and suicide risk - PubMed
Here's how to tell a psychopath from a sociopath
https://www.quora.com/Where-is-the-line-drawn-between-a-sociopath-and-a-psychopath/answer/Athena-Walker
The MAOA link is fascinating to me though it makes sense. I've had DNA tests done and I am within the 'normal' range for the gene.
Things which lead me to believe that there's a possibility that I am a psychopath are my total lack of empathy and remorse combined with a flat affect for most all other emotions however the oxytocin resistance along with responses to drugs made me curious. I am on TRT and the clinic offered oxytocin as a libido enhancer. My girlfriend was strongly effected but it did nothing at all for me. Later after I'd had some surgery I discovered that I had no addictive response to the opioids I'd been given.
Anyway, all the different contributing factors undoubtedly cause the spectrum of psychopaths that range from surgeons who save lives to monster who are locked up 23 hours a day in a supermax prison
Homeostasis.
I think that's the line - and that ties in quite neatly with the remarks I commented yesterday.
https://www.scientificamerican.com/article/what-is-homeostasis/
Factor 1 Psychopaths have homeostasis, and *have always had it* from their first breath, since their emotional apparatus does not have enough power to disrupt their Mind-Emotions-Body(Feelings) continuum.
They have therefore always find it rather easy to keep emotions in check, and use them to best advantage.
They will be also naturally inclined to have a reasonable balance of mind and body that will ward them off from such things as depressions, anxieties and
obesities.
They will tend to have good physical health overall, but they will also tend to die from sudden illness because they are naturally stubborn regards the idea of submitting themselves to the hands of doctors and medical institutions whose aptitude they won't naturally be inclined to trust.
They will rather trust their own bodies, since they've known them for a very long time.
They also trust their own mind over anyone else's, since it has always worked for them, and never against.
Their minds and bodies work in synch by default since forever = homeostasis.
Factor 2 Sociopaths, on the other hand - actually have their entire predicament derived from the fact that *they lost homeostasis* as an intrinsic part of their condition and adaptation.
So their behavior gets dysregulated. So does their thinking. So do their emotions. So does their bodies.
They will be therefore overrepresented in statistics regarding the leading causes of death, worldwide.
They will tend to have poor health overall, as well as extremes of neurosis or psychosis, depending on which polarity of the mind-emotions-body is running the show.
Unlike factor 1, factor 2's will be very likely to not only seek medical attention, but to be nagging towards doctors in pushing them to "just fix my body, man".
These are facts that can be easily looked up, it's no mere speculation.
It all boils down to homeostasis - or the lack there of.
That's the line right there.